While Syracuse’s big hospitals make headlines, a staffing emergency is hollowing out the ERs and clinics that rural CNY depends on — and a new federal budget just made it worse.
Drive 30 minutes in any direction from Syracuse and the healthcare landscape changes fast. The sprawling campuses of Upstate University Hospital and Crouse Health give way to smaller facilities — community hospitals with 50 to 160 beds, ERs staffed by a skeleton crew, and family health centers where one physician covers an entire county.
Those facilities are in trouble. And nobody in Central New York is talking about it.
The Staffing Numbers Are Brutal
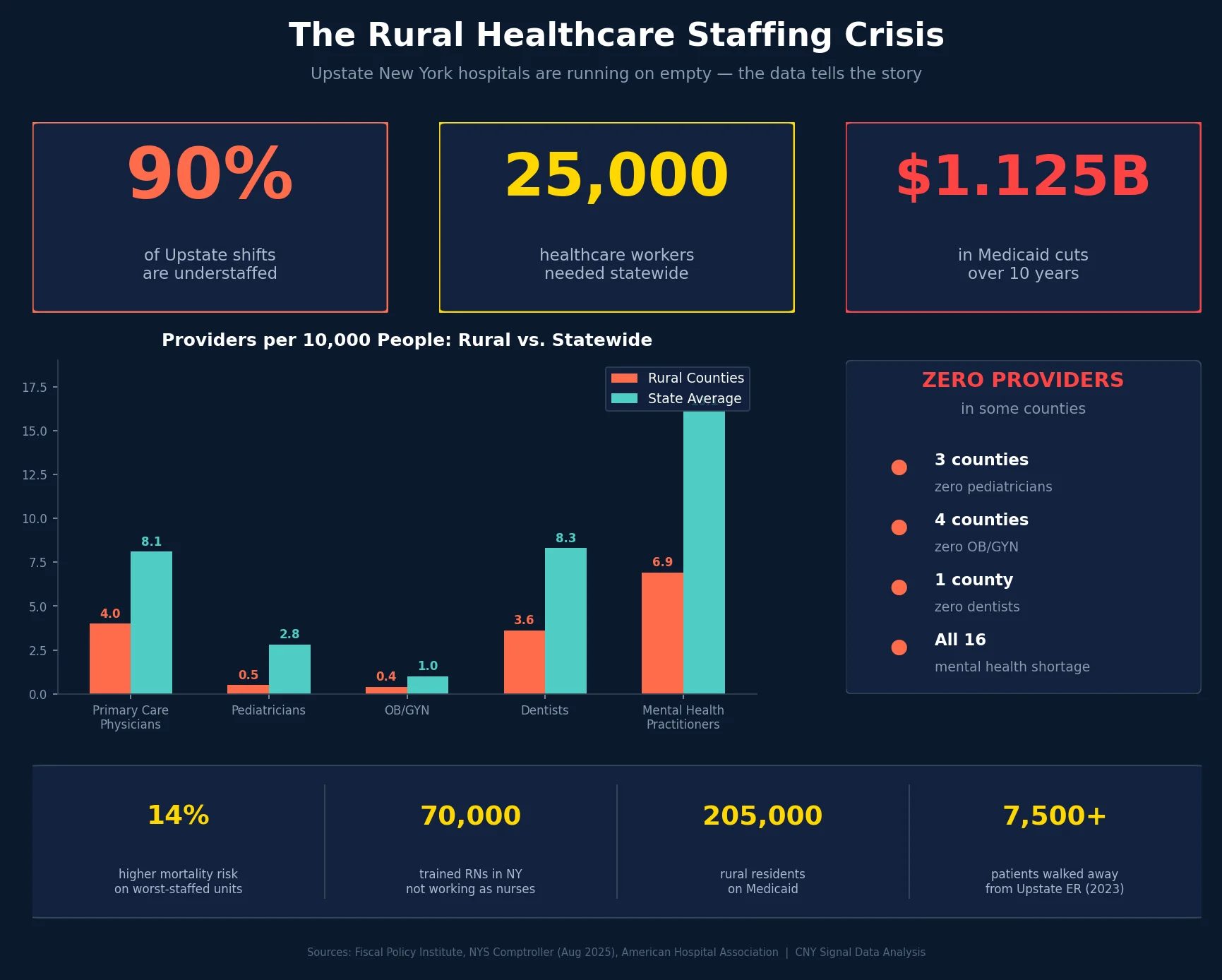
A December 2024 report from the Fiscal Policy Institute found that 90% of Upstate New York hospital shifts are currently understaffed. The gap is staggering: the state needs an additional 5,000 registered nurses and 20,000 ancillary staff — 25,000 healthcare workers total — to achieve safe staffing levels at Upstate facilities.
The consequences aren’t abstract. Chronic understaffing correlates with a 14% rise in mortality risk for patients on the worst-staffed hospital units — roughly 280 additional patient deaths per 100,000 hospitalizations.
Meanwhile, 70,000 trained RNs in New York are not currently working as nurses — more than 35% of all trained RNs in the state. They’ve left the profession for better pay, better hours, or less burnout. And despite the 2021 Clinical Staffing Committee Law taking effect in 2022, which was supposed to fix this, near 90% of shifts remain understaffed.
The Rural Picture Is Worse
In August 2025, NYS Comptroller Thomas DiNapoli released an audit of healthcare access in 16 rural counties across New York. The findings paint a picture of a system in slow-motion collapse:
- Primary care physicians: Rural counties average just 4 per 10,000 people, compared to 8.1 statewide and 8.4 nationally. The recommended guideline is 6.9 per 10,000.
- Pediatricians: Rural counties have 0.5 per 10,000 people, versus 2.8 statewide. Three counties have zero pediatricians.
- OB/GYN: Rural ratio is 0.4 per 10,000 — one physician for every 23,000 people. Four counties have no OB/GYN at all: Hamilton, Herkimer, Schuyler, and Yates.
- Dentists: 3.6 per 10,000 versus 8.3 statewide. Hamilton County has zero dentists.
- Mental health practitioners: 6.9 per 10,000 versus 16.1 statewide. All 16 counties are designated as shortage areas.
In the lowest-shortage areas examined, the physician ratio drops to 0.12 per 10,000 people — essentially no accessible primary care. About 173,000 people (23% of these counties’ population) live in federally designated Health Professional Shortage Areas for primary care alone.
What This Means for CNY
The Comptroller’s audit focused on 16 counties — Allegany, Cattaraugus, Chenango, Delaware, Essex, Franklin, Greene, Hamilton, Herkimer, Lewis, Schuyler, Steuben, Sullivan, Washington, Wyoming, and Yates. Several of those border the greater CNY region, and the dynamics are identical in the rural stretches of Madison, Cortland, Cayuga, and Oswego counties.
Community Memorial Hospital in Hamilton (Madison County) — a small community hospital with ER and primary care services — recently brought in a new CEO with three decades of experience at Oswego Health to try to stabilize operations. The hospital serves Hamilton, Morrisville, Cazenovia, Munnsville, and Waterville through five health centers, an urgent care clinic, and a 24/7 emergency department.
If you’re a farmer in Morrisville having a cardiac event at 2 a.m., the difference between a functional local ER and one that’s diverted or understaffed is the difference between a 10-minute ambulance ride and a 40-minute one to Syracuse. That’s not hypothetical. That’s the math.
Even in Syracuse itself, the crisis is visible. Upstate University Hospital has the second-longest ER wait time of all hospitals of its kind in New York State. More than 7,500 patients walked away from the Upstate ED in 2023, unable to get care — a crisis that began during COVID-19 and never recovered. Governor Hochul has since fully funded an ER overhaul at Upstate, but construction takes years.
The Federal Budget Made It Worse
The recently enacted federal budget bill (Public Law No: 119-21) includes Medicaid cuts that will hit rural New York hospitals hardest. According to the American Hospital Association, the law reduces federal Medicaid spending on New York’s rural hospitals by $1.125 billion over 10 years.
It also reduces eligibility for Medicaid and the Essential Plan — critical lifelines for rural hospitals where a disproportionate share of patients rely on public insurance. In the 16 rural counties examined by the Comptroller, 27% of the population — roughly 205,000 people — were enrolled in Medicaid as of May 2025.
New York has six rural hospitals in the top 10% nationwide for their Medicaid payer mix, and five more have had negative margins for three consecutive years. When you cut Medicaid reimbursement to facilities that already operate on razor-thin margins, you don’t get efficiency — you get closures.
Nationally, 29 rural hospitals face immediate risk of closure due to financial distress, according to Saving Rural Hospitals data. The federal bill does earmark $50 billion from 2026 to 2030 for a Rural Hospital Transformation Program, but there’s no guarantee New York will see significant funding — and new student loan limits of $50,000 annually for professional students (with a $200,000 aggregate cap) will make it even harder to attract physicians to rural areas through loan forgiveness programs.
What Needs to Happen
The solutions aren’t mysterious — they’re just expensive and politically difficult:
- Recruitment pipelines: Training programs specifically designed for rural care delivery, with service commitments tied to loan forgiveness that actually works under the new caps.
- Telemedicine and remote specialty support: Rural ERs don’t need every specialist on-site, but they need real-time access to ones in Syracuse.
- New staffing models: The traditional model of long on-call hours is driving clinicians away. Flexible, team-based approaches could fill gaps without burning people out.
- Medicaid rate increases: Until rural hospitals can cover costs, they’ll continue cutting services and losing staff.
Ten of the 16 rural counties in the Comptroller’s study are federally designated Health Professional Shortage Areas in primary care, dental, and mental health. All 16 have shortage designations in at least two medical fields. The designation exists. The funding to fix it doesn’t — yet.
If you’ve experienced ER diversions, long wait times, or service cuts at a rural CNY hospital, CNY Signal wants to hear from you. Email [email protected].